Single-Payer Health Care: A Tale of 3 States



What do Vermont, the bluest of blue states, Colorado, a purple-trending blue state, and Massachusetts, home of an all-blue congressional delegation, have in common? They’ve all failed at pursuing single-payer.
States are the laboratories of democracy. Yet, single-payer initiatives have consistently failed. These experiments demonstrate the challenges that single-payer faces—ranging from high costs to opposition from core progressive constituencies. This report examines the single-payer experience in each of the three states. It also looks at what rose from the ashes after the efforts failed and what policymakers can learn.
Plan Summaries
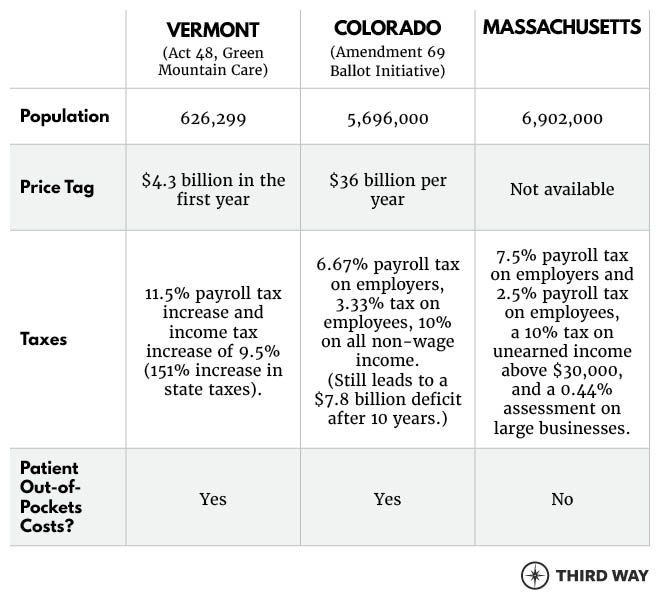
Vermont, Colorado, and Massachusetts each took a different approach toward single-payer, as depicted in the chart below.1
Vermont
In 2011, Vermont State Senator Peter Shumlin became governor having campaigned on single-payer health care. The enactment of the ACA in the previous year made single-payer a seemingly realistic option because the law allowed states to establish innovative ways to finance and deliver health care. In his first year in office, Governor Shumlin took the state one step closer to single-payer by winning the enactment of legislation to create the nation’s first single-payer system, called Green Mountain Care. His attempts to implement the law spanned his first two terms in office (Vermont governors serve two-year terms) during which he continued to campaign on single-payer right up to his election to a third term. Despite all the momentum, Shumlin could not overcome several major obstacles, and the single-payer experiment officially ended in late 2014.
What were the obstacles and why did they prove immovable?
-
Escalating costs. The initial estimate for Green Mountain Care was that it would save $1.6 billion over ten years. However, there were still numerous unknowns, such as what benefits patients would receive and their specific cost-sharing requirements.2 Once enacted, Governor Shumlin had until January 2013 to present a financing package to state lawmakers that would pay for the new single-payer health care system. However, that deadline came and went. Nonetheless, the governor pushed ahead without a plan to pay for the legislation. “We can move full speed ahead with what we need without knowing where the money’s coming from,” said the Governor’s special counsel for health reform.3 Nearly a year later, the Governor announced he would release a new financing plan after the 2014 elections.
The Governor’s team ran 14 financing concepts that tried to create a fair balance between payroll taxes and income taxes. But, the computer models all showed that the only way to set taxes at rates as low as they wanted would be to give residents skimpier coverage that most insured Vermonters already had. “We were pretty shocked at the tax rates we were going to have to charge,” Governor Shumlin recalled.4 After it was all said and done, Green Mountain Care would have cost $4.3 billion in its first year—financed, in part, by $2.8 billion in new state tax revenue, or a 151% increase in total state taxes.5 Governor Shumlin’s team estimated this cost would have swollen to over $5 billion in 2021. For context, the entire budget for the state of Vermont was $5.01 billion for 2012-2013. Officials in the state determined that an 11.5% state payroll tax and a 9.5% income tax would be necessary to pay for the new health care system. “In a word, enormous,” is how Governor Shumlin described the tax hikes needed to fund single-payer.6 “As we completed the financing modeling,” Shumlin lamented, “it became clear that the risk of economic shock is too high to offer a plan I can responsibly support…”7 Despite being a small, progressive state, the government still could not figure out a way to make the numbers work.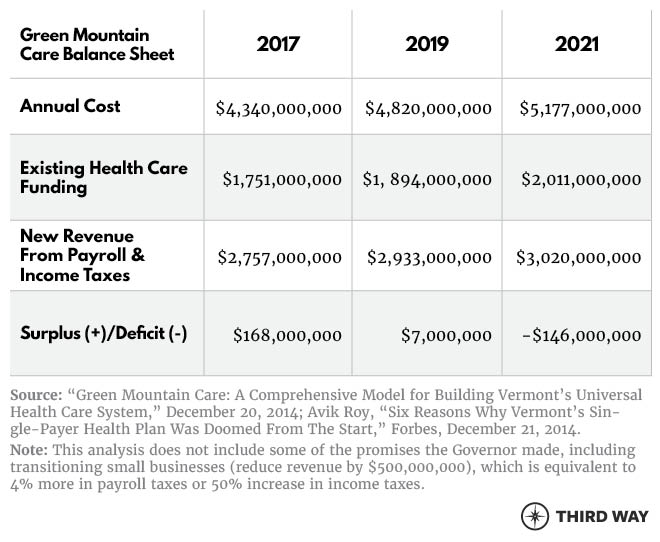
-
Fragmented coalitions. Union members, community activists, disability rights advocates, and the Vermont Workers’ Center (a group of single-payer supporters) all initially rallied to support the legislation. However, the new law unleashed a torrent of lobbying by these organizations trying to ensure the new law benefited their members before the new health care system was set to be implemented in 2017. single-payer advocates and unions pressed hard for generous benefits. Employers wanted coverage for out-of-state employees, while small businesses were terrified of huge tax increases. Large businesses pushed back strongly on the cost of the new plan.8 Self-insured companies lobbied against tax increases, as they resented the prospect of being taxed more to help others get coverage. These groups also failed to educate the public on the trade-offs a single-payer system would entail, including the huge tax increases.
Governor Shumlin said that no one should be worse off under his plan, so he agreed the new system should cover out-of-state workers and 94% of Vermonters’ health care costs, more than the most generous plan available on the marketplace today.9 He also agreed to consider a grace period for new taxes on small businesses, which would have reduced funding for the program by another $500 million. Still, these decisions made paying for the plan even harder. As a result, a few months before the decision about whether to move ahead, the Vermont public was divided over single-payer: 40% support, 39% opposed, and 21% undecided.10 Support had fallen from the initial level of 48% support, 36% opposed, and 16% undecided.11 - Regressive impact on families. Nearly all private employers, but particularly small businesses, would pay more under the new health plan. The taxes required to provide the coverage Governor Shumlin promised would have shifted costs onto employers, who could then shift those costs onto their employees. While many employees would receive better coverage under this new plan, other employees faced a new financial burden as these new costs would likely come out of their wages. For example, a worker making $20,000 at a small firm would be worse off under the new plan.12
With single-payer dead in the state, Vermont switched gears and pursued an innovative delivery model that built on the ACA instead of replacing it. In October 2016, Governor Shumlin and the Green Mountain Care Board—the board originally responsible for implementing single-payer—released the first draft of the Vermont All-Payer Accountable Care Organization (ACO) Model, which pilots new payment models that coordinate physical health, mental health, and social services to help patients with the most complex needs. The new All-Payer ACO Model successfully builds on the existing health care infrastructure and state partners instead of trying to re-make the entire health system. Initial results from the study show that Medicaid beneficiaries are making greater use of primary care and behavioral health services, and those individuals deemed “high or rising risk” had substantially fewer emergency department visits than before the program.13
Colorado
In 2016, Colorado residents voted on a citizen-initiated single-payer ballot initiative, Amendment 69. The ballot initiative would have amended the state constitution and created a taxpayer-funded, universal health plan for the state that would be operated by a 21-person elected board. This would have put all Colorado residents who currently receive private insurance onto ColoradoCare, while those with Medicare and Tricare would keep that insurance.14 ColoradoCare would cover 11 categories of health services, such as “prescription drugs and medical equipment” and “preventive and wellness services,” with no deductibles or copayments for preventive and primary care services and some cost-sharing for other services. Despite being a progressive policy proposal, many Democrats and progressives opposed the measure. With close to 2 million votes, Amendment 69 was strongly defeated by nearly 60% (79% opposed, 21% in favor).15 Not one county in Colorado voted in favor of the initiative. 16 Even in some of the most liberal counties that voted in favor of Hillary Clinton by a large majority, the ballot initiative failed by at least 20%.17 This same failure was seen in other progressive states as well. California’s ballot initiative garnered only 27% of the vote and Oregon’s initiative saw only 20% in favor.18

Why did the ballot initiative get defeated by such large margins?
-
Escalating costs. The ballot initiative would have resulted in a $25 billion tax hike in the first year in order to fund the $36 billion health care program, which is nearly $10 billion larger than the 2017 budget for the entire state.19 Financing for the new health care system was a 10% tax on nonwage income and a 6.67% payroll tax on employers and 3.33% tax on employees.20 Even with these new taxes, the state would face a $7.8 billion deficit after ten years.
Colorado voters hadn’t passed a statewide tax hike for more than two decades, making the proposal a hard sell. Some voters worried that the price tag would make Colorado less attractive to new businesses and young workers.21 Voters were also concerned about the proposed tax authority the law would give to the new 21-member governing board. The board would have the ability to raise taxes with very little oversight. If health costs increased or the plan was more expensive than the models showed, the board would be forced to find a way to pay for it, primarily by raising taxes further. The law also had no way to ensure transparency on the board. One resident noted that it would be very easy for a donor to influence the makeup of the board and dictate the success of the new health care system.22 This unorthodox transfer of taxing power with no oversight gave many voters pause. - Fragmented coalitions. Amendment 69 was opposed by dozens of organizations across the political spectrum. Progressive think tanks, unions, the business community, and advocacy groups, came out against the measure because it was “a poorly thought-through initiative.”23 Women’s health groups, including NARAL and Planned Parenthood, opposed the bill because it would remove access to abortion for the hundreds of thousands of women currently in private health plans that cover the procedure. Due to a 1984 Colorado law banning public funds from paying for abortions, the proposed bill would not be able to cover elective abortions for any woman in the state. As amendments can only address one issue, the ballot initiative could not make any changes to the existing abortion law.24 Moderate policymakers such as Governor John Hickenlooper, Senator Michael Bennet, and former Governor Bill Ritter all came out against the bill. This outcry led to citizens’ negative perception of the bill. In an August 2016 poll, 27% supported and 65% opposed Amendment 69. Democrats were more favorable toward the measure, with 41% in support and 45% in opposition.25
- Regressive impact on families. A report by the left-leaning Colorado Fiscal Institute noted that while many low-income Hispanic families would pay less under ColoradoCare (not counting the employer side of the payroll tax), poor Medicaid enrollees would be faced with new taxes without new health benefits to offset them.26 Similar to the legislation in Vermont, low-income workers would disproportionately bear the burden of costs in a health care system financed on payroll taxes, while receiving coverage that would be no better than what they already had.
While gubernatorial candidate Jared Polis called for a multi-state single-payer system on the campaign trail, after his election, he instead has focused on lowering health care costs for Coloradans.27 In April 2019, Governor Polis unveiled the Roadmap to Savings Coloradans Money on Health Care. The plan included passing a public option, a reinsurance program, a ban on surprise billing, expanding the primary care workforce, and increasing access to healthy food. His first action was to sign House Bill 1001, which requires financial transparency of hospitals.28
Massachusetts
Massachusetts has a longer, more complicated single-payer story, but the ending was the same. The state has debated the single-payer idea for three decades, with the first single-payer bill being introduced in 1986. Local, non-binding ballot initiatives in support of single-payer have been passed over 20 times.29 The state also has some of the strongest advocates for single-payer. Yet, despite the support from constituents and legislative interest, the bill has never gotten out of committee, let alone made it to the governor’s desk. Furthermore, candidates who have run on a single-payer platform, such as the former acting administrator of the Centers for Medicare and Medicaid Services Donald Berwick, have not won elections.30 Despite public support, legislative action, and a strong progressive coalition, single-payer has never gotten off the ground. Why not?
Similar to the other two states, the taxes necessary to fund a single-payer bill would be huge. MassCare, a Boston-based advocacy group, estimated that single-payer could be financed with a 10% capital gains tax on unearned income above $30,000, and a payroll tax of 7.5% for employers and 2.5% for employees.31 The state’s fiscal 2019 budget totals $41.2 billion, which includes all the money used to pay for public services like fixing roads and funding schools. About 40% already goes toward public insurance programs. Adding $22.8 billion in health costs (the amount currently paid by private insurance) would increase the state budget by more than 50%.32
John McDonough, a professor of public health at Harvard T.H. Chan School of Public Health said the biggest issue facing Medicare for all is related to cost. “How are you going to pay for it?” he asked, rhetorically. “The level of taxation that would be required to replace private premiums would be seen as off the wall by most people.” Furthermore, health care costs in Massachusetts have been increasing rapidly. In the last five years, health care costs grew 21%, increasing to $61.1 billion in 2017 compared to $50.5 billion in 2013. “It’s almost impossible to find a revenue source that grows at the rate you would need to feed moderate cost growth in the health care system,” said Anya Rader Wallack, a professor in the School of Public Health at Brown University in Rhode Island.33
While single-payer has continued to stall for decades, the state has pushed forward on health care in a multitude of ways. Massachusetts passed a health care reform law in 2006 with the aim of providing health insurance to nearly all of its residents. The law mandated that nearly every resident of Massachusetts obtain a minimum level of insurance coverage, provided free and subsidized health care insurance for low-income residents, and mandated most employers to provide healthcare insurance. Many provisions of the law, such as the Massachusetts Health Connector, were used in the drafting of the ACA. 34 After the law’s implementation, 97% of Massachusetts residents had health coverage compared to just over 90% nationally.35 The reform also improved health outcomes: the state saw reduced mortality for all residents. The mortality rate decreased even more among low-income households and those who were previously uninsured.36

Conclusion
Single-payer advocates are right that universal coverage is fundamental to a successful health care system, economy, and country. However, as these states have shown, raising taxes to unprecedented levels and upending the entire health care system is not popular. So what is the alternative?
First, Congress needs to address the costs of health care. No one should go bankrupt from a hospital visit, and everyone should have access to care they can afford. But as Vermont learned, simply replacing premiums with taxes would require a huge payroll tax of between 10-25%. Further, the “taxes instead of premiums” message has failed in states from Colorado, to California, to Vermont. For example, in California, 53% of likely voters back single-payer but support drops to just 41% when they are told it will require new taxes.
Instead, let’s expand on a technique from the ACA: cap out-of-pocket costs based on income no matter where the person gets insurance. This cap can be used in Medicare, Medicaid, and private insurance so that no middle-class person would pay more than 10% of their income on health care costs.
Furthermore, the right coalitions must be in the room. Those coalitions need to be comprised of the people who use and pay for their health care. A massive coalition of consumers, unions, employers, small businesses, governors, and willing participants of the health care industry are needed to overcome opposition to change. The kernels of such a coalition are available through Consumers First, which is focused on realigning health care incentives to lower costs and improve quality.37
Third, any health policy plan must avoid a regressive impact on low-income families. A consultant on the Vermont single-payer plan said, “If you can’t do it in Vermont, with one private health plan and low uninsured rates, then the amount of disruption you would have nationally with winners and losers would be enormous.”38 Some people in this country receive free or incredibly discounted care through Medicaid and the ACA exchanges. However, under a single-payer plan where taxes are increased upwards of 10%, they would bear an undue cost burden. Instead of making them worse off, Congress should focus on the millions of people who are eligible for free and discounted care and make sure they are enrolled through auto-enrollment or one-click simplified enrollment process. And all low- and middle-income families should receive protection from high costs based on their income.39
Let’s learn from the single-payer experiments in these states. With 29 million uninsured and tens of millions more worried about health care costs, the country does not have time to waste on policies that won’t go anywhere. Instead, let’s strengthen the ACA, control costs, build strong coalitions, and achieve universal coverage.
Endnotes
Governor Peter Shumlin to the Vermont State Legislature, “Green Mountain Care: A Comprehensive Model for Building Vermont’s Universal Health Care System,” December 20, 2014. Accessed July 15, 2019. Available at: https://hcr.vermont.gov/sites/hcr/files/pdfs/GMC%20FINAL%20REPORT%20123014.pdf; Henry Schwan, “Single-payer health insurance: discussion heats up in Massachusetts,” The MetroWest Daily News, June 10, 2019. Accessed July 15, 2019. Available at: https://www.metrowestdailynews.com/news/20190610/single-payer-health-insurance-discussion-heats-up-in-massachusetts; United States, Massachusetts State Senate, “S.683-- An Act Establishing Medicare for All in Massachusetts,” 191th Congress, 1st Session, January 22, 2019. Accessed July 15, 2019. Available at: https://malegislature.gov/Bills/191/SD2062; “ColoradoCare: An Independent Analysis,” Colorado Health Institute, 2016. Accessed July 15, 2019. Available at: https://www.coloradohealthinstitute.org/research/coloradocare-independent-analysis
Amy Goldstein, “Why Vermont’s single-payer effort failed and what Democrats can learn from it,” The Washington Post, April 29, 2019. Accessed July 15, 2019. Available at: https://www.washingtonpost.com/national/health-science/why-vermonts-single-payer-effort-failed-and-what-democrats-can-learn-from-it/2019/04/29/c9789018-3ab8-11e9-a2cd-307b06d0257b_story.html?utm_term=.0f1f772cabd6
Avik Roy, “Six Reasons Why Vermont's Single-Payer Health Plan Was Doomed From The Start,” Forbes, December 21, 2014. Accessed July 15, 2019. Available at: https://www.forbes.com/sites/theapothecary/2014/12/21/6-reasons-why-vermonts-single-payer-health-plan-was-doomed-from-the-start/#42b3bcf14850
Amy Goldstein. “Why Vermont’s single-payer effort failed and what Democrats can learn from it.”
Avik Roy, “Six Reasons Why Vermont's Single-Payer Health Plan Was Doomed From The Start.”
Bruce Parker, “Shumlin: Single-payer ‘greatest disappointment of my political life,’” Sun Community News, December 18, 2014. Accessed July 15, 2019. Available at: https://www.suncommunitynews.com/articles/the-sun/shumlin-single-payer-greatest-disappointment-my-po/
Amy Goldstein. “Why Vermont’s single-payer effort failed and what Democrats can learn from it.”
Steve Early, “Vermont’s Struggle for Single-Payer Healthcare,” The Nation, March 10, 2011. Accessed July 15, 2019. Available at: https://www.thenation.com/article/vermonts-struggle-single-payer-healthcare/
Avik Roy, “Six Reasons Why Vermont's Single-Payer Health Plan Was Doomed From The Start.”
Morgan True, “VTDigger/Castleton Poll: Vermonters split on single payer,” VT Digger and Castleton, April 23, 2014. Accessed July 15, 2019. Available at: https://vtdigger.org/2014/04/23/vtdiggercastleton-poll-21-percent-seem-confused-term-single-payer/
Poll, Castleton Polling Institute, May 2012. Accessed July 15, 2019. Available at: https://www.castleton.edu/academics/undergraduate-programs/political-science/poll-results/may-2012-poll-results/
Governor Peter Shumlin to the Vermont State Legislature, “Green Mountain Care: A Comprehensive Model for Building Vermont’s Universal Health Care System,” December 20, 2014. Accessed July 15, 2019. Available at: https://hcr.vermont.gov/sites/hcr/files/pdfs/GMC%20FINAL%20REPORT%20123014.pdf
Martha Hostetter, Sarah Klein, and Douglas McCarthy, “Vermont’s Bold Experiment in Community-Driven Health Care Reform,” The Commonwealth Fund, May 10, 2018. Accessed July 15, 2019. Available at: https://www.commonwealthfund.org/publications/case-study/2018/may/vermonts-bold-experiment-community-driven-health-care-reform?redirect_source=/publications/case-studies/2018/may/onecare-vermont
John Daley, “Coloradans Will Put Single-Payer Health Care To A Vote,” National Public Radio, December 19, 2015. Accessed July 15, 2019. Available at: https://www.npr.org/sections/health-shots/2015/12/19/458688605/coloradans-will-put-single-payer-health-care-to-a-vote
Secretary of State Wayne Williams, “Colorado Election Results,” November 8, 2016. Accesses July 15, 2019. Available at: http://results.enr.clarityelections.com/CO/63746/184388/Web01/en/summary.html
“Colorado Amendment 69 — Create State Healthcare Systems — Results: Rejected,” The New York Times, August 1, 2017. Accessed July 15, 2019. Available at: https://www.nytimes.com/elections/2016/results/colorado-ballot-measure-69-state-healthcare-system
“Colorado Results,” The New York Times, August 1, 2017. Accessed July 15, 2019. Available at: https://www.nytimes.com/elections/2016/results/colorado
Eli Sherman, “Medicare for all: An empty promise in Massachusetts?” Wicked Local, October 29, 2018. Accessed July 15, 2019. Available at: https://www.wickedlocal.com/news/20181022/medicare-for-all-empty-promise-in-massachusetts
John Ingold, “ColoradoCare measure Amendment 69 defeated soundly,” The Denver Post, November 8, 2016. Accessed July 15, 2019. Available at: https://www.denverpost.com/2016/11/08/coloradocare-amendment-69-election-results/; Marianne Goodland, “What’s in the proposed 2017-2018 state budget for the average Coloradan,” The Colorado Independent, March 27, 2017. Accessed July 15, 2019. Available at: https://www.coloradoindependent.com/2017/03/27/2017-2018-state-budget-preview/
“ColoradoCare: An Independent Analysis.”
John Daley, “Coloradans Will Put Single-Payer Health Care To A Vote.”
Kelsey Ray, “ColoradoCare suffered a whopping defeat. Here’s why.” The Colorado Independent, November 8, 2016. Accessed July 15, 2019. Available at: https://www.coloradoindependent.com/2016/11/08/coloradocare-amendment-69/
Dylan Matthews, “Single-payer health care failed miserably in Colorado last year. Here’s why.” Vox, September 17, 2017. Accessed July 15, 2019. Available at: https://www.vox.com/policy-and-politics/2017/9/14/16296132/colorado-single-payer-ballot-initiative-failure; Bruce Japsen, “Colorado Rejects Single-Payer Healthcare Insurance,” Forbes, November 6, 2016. Accessed July 15, 2019. Available here: https://www.vox.com/policy-and-politics/2017/9/14/16296132/colorado-single-payer-ballot-initiative-failure
“Ballot History,” Colorado State Legislature, 1984. http://www.leg.state.co.us/lcs/ballothistory.nsf/835d2ada8de735e787256ffe0074333d/6f17c468971b2fc387256ffd006a496e?OpenDocument
David Flaherty, “Amendment 69, ColoradoCare Survey Findings,” Magellan Strategies, September 6, 2016. Accessed July 15, 2019. Available here: https://magellanstrategies.com/amendment-69-voter-opinion-survey/
Bruce Japsen, “Colorado Rejects Single-Payer Healthcare Insurance.”
John Herrick, “Ask the Indy: What’s going on with universal health care in Colorado?” The Colorado Independent, February 26, 2019. Accessed July 15, 2019. Available at: https://www.coloradoindependent.com/2019/02/26/ask-the-indy-universal-health-care-single-payer/
Joe Hanel, “Governor Polis Unveils Grand Plan for Health,” Colorado Health Institute, April 4, 2019. Accessed: July 15, 2019. Available at: https://www.coloradohealthinstitute.orF7.8g/blog/governor-polis-unveils-grand-plan-health
Benjamin Day, “Ben’s Testimony for Single Payer in Massachusetts,” Healthcare-NOW!, March 22, 2016. Accessed July 15, 2019. Available at: https://www.healthcare-now.org/blog/healthcare-nows-testimony-for-massachusetts-single-payer-bills/
John McDonough, “The Demise of Vermont’s Single-Payer Health Care Plan,” Medium, August 22, 2017. Accessed July 15, 2019. Available at: https://medium.com/@pplswar/the-demise-of-vermonts-single-payer-health-care-plan-b62c4746c93d
Henry Schwan, “Single-payer health insurance: discussion heats up in Massachusetts,”
Eli Sherman, “Medicare for all: An empty promise in Massachusetts?”
Eli Sherman, “Medicare for all: An empty promise in Massachusetts?”
Maura Calsyn, “Romneycare Versus Obamacare,” Center for American Progress, July 31, 2012. Accessed July 15, 2019. Available at: https://www.americanprogressaction.org/issues/healthcare/reports/2012/07/31/11946/romneycare-versus-obamacare/
“2018 Annual Health Care Cost Trends Report,” Massachusetts Health Policy Commission, February 2019. Accessed July 15, 2019. Available at: https://www.mass.gov/files/documents/2019/02/20/2018%20Cost%20Trends%20Report.pdf
Dr. Benjamin Sommers, Dr. Sharon Long, Dr. Katherine Baicker, “Changes in Mortality After Massachusetts Health Care Reform: A Quasi-experimental Study,” Annals of Internal Medicine, May 6, 2014. Accessed July 15, 2019. Available at: https://annals.org/aim/article-abstract/1867050/changes-mortality-after-massachusetts-health-care-reform-quasi-experimental-study
“Consumers First,” FamiliesUSA. Accessed July 15, 2019. Available at: https://familiesusa.org/initiatives/consumers-first
Amy Goldstein. “Why Vermont’s single-payer effort failed and what Democrats can learn from it.”
David Kendall, Gabe Horwitz, and Jim Kessler, “Cost Caps and Coverage for All: How to Make Health Care Universally Affordable,” Third Way, February 19, 2019. Accessed July 15, 2019. Available at: https://www.thirdway.org/report/cost-caps-and-coverage-for-all-how-to-make-health-care-universally-affordable
Subscribe
Get updates whenever new content is added. We'll never share your email with anyone.