Report Published November 18, 2015 · Updated November 18, 2015 · 18 minute read
Coordinate Care for the Most Vulnerable


No one expects to have a heart attack—but when it happens, most are overwhelmed, scared, and simply hoping to survive. If you’re fortunate enough to live, you may face another serious challenge dealing with medical bills and rehabilitation coverage. Imagine having a heart attack every year for four years, and having two health plans both deny coverage for proper preventative treatment. That’s what happened to M.C. Kim. After four heart attacks over the course of four years, he took the initiative to find a cardiac rehabilitation program that would teach him how to reduce his chances for another heart attack. Instead of receiving coverage, his Medicare office told him to call Medicaid, his Medicaid office told him to call Medicare, and Kim was eventually denied coverage for this program. Kim recalls, “I was like a ping pong ball … nobody wanted to take responsibility.”1
Better coordination of care may have prevented some of Kim’s 20 trips to the emergency room over a six-year period. In order to encourage coordination and coverage of Kim’s program, either Medicare or Medicaid needs to take responsibility for coordinating all the necessary services for those dually eligible for both programs. This coordination would have encouraged coverage of Kim’s cardiac rehabilitation program—and decreased or prevented his future emergency room visits. Coordinating care for dual eligibles can help patients like M.C. Kim get coverage for necessary treatment programs and can save the federal government $38.9 billion over ten years.
This idea brief is one of a series of Third Way proposals that cuts waste in health care by removing obstacles to quality patient care. This approach directly improves the patient experience—when patients stay healthy, or get better quicker, they need less care. Our proposals come from innovative ideas pioneered by health care professionals and organizations, and show how to scale successful pilots from red and blue states. Together, they make cutting waste a policy agenda instead of a mere slogan.
What is Stopping Patients from Getting Quality Care?
Of the nine million Americans who are dually eligible for Medicare and Medicaid, more than half are female, suffer from three or more chronic health conditions, and don’t have full mental or cognitive abilities.2 Forty-four percent cannot live on their own without assistance.3 Nearly nine of every 10 live below 150% of the federal poverty level.4 Although they make up only 20% of the Medicare beneficiaries in the traditional fee-for-service plan, dual eligibles are responsible for 31% of Medicare spending.5 In Medicaid, their 15% representation comprises 39% of total spending.6 Dual eligibles are more likely to be in poor, or only fair, health when compared to the rest of the Medicare population by a margin of 49% to 22%. They are also more likely to be hospitalized by a margin of 26% to 18%.7
Dual eligibles face many challenges due to poor health conditions, low-incomes and other issues related to their socioecomic status. Their care is also impeded, however, by an antiquated financing and benefit structure divided between Medicare and Medicaid. Medicare covers most acute care services (e.g., physicians, hospitals, lab tests, and prescriptions) and some long-term care support services (e.g., nursing homes and home care).8 Medicaid covers most long-term care services, provides some services for which Medicare has only limited coverage (e.g., vision, dental, and transportation), and is responsible for some, or all, Medicare premiums and cost sharing.9 With this fragmentation, a dually eligible beneficiary can have as many as three entities responsible for their coverage: a state Medicaid program or managed care plan, the Medicare program or Medicare Advantage plan, and a stand-alone Medicare Part D Prescription Drug plan.
The only point of convergence between Medicare and Medicaid in the fee-for-service system has historically has been the beneficiaries themselves, who often do not have the ability to navigate and coordinate the various sources of coverage. There is no comprehensive plan to integrate the multiple sources of financing and coordinate benefits across the programs, each with their often-complex sets of coverage rules for even basic items like a walker. Although Medicare Advantage Dual Eligible Special Needs Plans, which do provide care coordination, are available in some areas of the country, their total enrollment is less than 100,000—a drop in the bucket considering the millions of duals.10 Other initiatives like social HMOs, Program of All-Inclusive Care for the Elderly (PACE), Managed Long Term Services and Supports, Medicare-Medicaid plans have also seen limited enrollment. Indeed, only 12.6% of care for dual eligible beneficiaries today is coordinated and integrated.11 Not surprisingly, the lack of integration and coordination in the fee-for-service system has produced significant confusion for beneficiaries and providers, resulting in highly inefficient use of services with over-utilization in some cases, gaps in care at other times, and lost opportunities to improve beneficiary health and quality of life.12
The incentives for either Medicare or Medicaid separately to coordinate care for patients are weak and inconsistent. Generally, each program lacks the financial incentives to adopt policies that reduce dual eligible costs paid for by the other. For example, Medicaid—and the nursing homes it funds—has a financial incentive to admit their dual eligible patients to the hospital after they have exhausted their Medicare-covered skilled nursing facility days because doing so will “restart the clock” on the Medicare episode of coverage. This leads to less exposure by the state to additional costs and higher reimbursement rates for the nursing home.13 Because Medicare payment rates are often higher than Medicaid’s, providers have significant incentives for finding similar ways of shifting costs from Medicaid to Medicare so they can receive higher reimbursements. That’s why studies show increases in Medicare-covered hospital services in states where Medicaid reimbursement for nursing facility care is below average.14
Even with stronger incentives to coordinate care, there would still be obstacles to integrate the multiple sources of financing. A state could have a contract with one health plan for Medicaid benefits, but a beneficiary could choose a different health plan for Medicare benefits. Health plans are generally prohibited from cross marketing to explain the benefits of having a service coordinator who can manage the complex rules of each program. Another hurdle is a state’s capacity to take on the task of integrating the financing. Most states would at least need a partner to assist with integration. Lastly, federal and state administrators would need a better relationship to trust that funds are being properly used, which would help reduce micromanagement.
Where Are Innovations Happening?
There are a number of innovative efforts happening across the country to help the duals.
Under contract with the state of Texas, Amerigroup, a private health plan, provides long-term care services to duals with coordinated care and integrated financing. It also has a Medicare Advantage Special Needs plan that enrolls many of the same duals. Together, they have reduced hospital costs by 22%, and emergency room use has decreased by 40%.15 Compared with the traditional, fee-for-service care, the Texas program has generated savings of 15% for acute outpatient care and 10% for long-term services and support.16
The North Carolina Community Care Network (NC-CCN) provides coordinated care but without the financing integration. NC-CCN is a primary care case management model used by the state to provide care coordination for its Medicaid program. It was expanded to cover dual eligible beneficiaries under the Medicare Health Care Quality (MHCQ) demonstration program, authorized in the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA).17
Under the program, NC-CCN assigns dual eligible beneficiaries to physician practices that are responsible for coordinating care and measuring outcomes.18 The state provides these practices with support, including community-based coordination services, and a host of data and analysis tools such as patient-level and provider-level quality reports. In addition, physicians are paid a monthly fee for providing care coordination services.19
The state is eligible for shared savings under the MHCQ program upon achieving quality targets.20 Performance in the first year of the NC-CCN demonstration was based on 18 quality measures covering management of areas such as diabetes, heart failure, and transitional care. The number of quality measures will expand over time.21
In the NC-CCN program, the state pays monthly case management fees to physicians up front which, absent the MHCQ demonstration, would not be reimbursable by Medicare. Yet, this investment by North Carolina Medicaid is making a marked difference in utilization of acute care services by the dual eligible population. Hospital inpatient admissions for the elderly, blind, and disabled dual eligible NC-CCN population was 15-20% lower than for the un-enrolled population. For NC-CCN enrollees with two or more chronic conditions, emergency room visits were 19% lower than the control population.22 NC-CCN reduced Medicaid spending by about $1 billion over four years and slowed the Medicare cost growth rate relative to a comparison group.23
States are also implementing care coordination models under the Centers for Medicare & Medicaid Services’ (CMS) State Demonstration to Integrate Care for Dual Eligible Individuals and the Capitated Financial Alignment Demonstration Initiative, with most demonstrations running for approximately three years.
For example, Massachusetts is focusing on full benefit dual eligible beneficiaries between the ages of 21 and 64. Using the capitated model, the state, CMS, and health plans have a three-way contract under which the health plan will coordinate and be accountable for all Medicare and Medicaid services. Called One Care: Mass Health plus Medicare, the state has set contracts with three different plans to integrate Medicaid and Medicare financing and provide person-centered, comprehensive Medicaid and Medicare benefits.24 In addition to voluntary enrollment by those eligible to participate, Massachusetts is conducting automatic assignment in a One Care plan in three rounds throughout the first year of implementation.25 Automatic assignment is restricted to four counties in which at least two One Care plans are available and excludes individuals enrolled in a Medicare Advantage plan or the PACE program. All beneficiaries retain the right to choose a different One Care plan or retain their prior Medicare and Medicaid options.26 As of August 1, 2015, 17,518 dual eligible beneficiaries were enrolled in one of three One Care plans.27 Approximately 115,000 full dual eligible adults ages 21-64 are included in the target population.28 Despite a rocky start, One Care is seeing high satisfaction rates among participants.29
How Can We Bring Solutions to Scale?
Congress should adopt policies to coordinate care and integrate coverage for dual eligible beneficiaries as well as align Medicare and Medicaid financing. By doing this, just one program takes responsibility for coordinating all the services the duals need, with opportunities for both programs to share in the accrued savings. Focus should begin with full benefit dual eligible beneficiaries, who are eligible for Medicaid long-term services due to disability and low-income. Eventually, coordinated coverage could be expanded to include partial dual eligible beneficiaries, who are not disabled but are eligible for financial assistance to cover Medicare’s out-of-pocket costs and premiums due to low-income.
CMS is currently testing ways for state and federal governments to partner with health plans and providers in integrating coverage for the duals through two programs: the State Demonstration to Integrate Care for Dual Eligible Individuals and the Capitated Financial Alignment Demonstration Initiative.30 Policymakers should take a number of steps to build up from this foundation:
These efforts should be expanded so that every dual eligible beneficiary in the country is covered by a care coordination program that also integrates financing sources, whether through private or public health plans. Approaches to health care and care coordination will vary for each beneficiary because the duals have very different needs and circumstances.31 Yet all beneficiaries have a great need for increased coordination.
Each care coordination model should incorporate methods that have been proven successful in other settings and that are tailored to sub-categories of dual eligible beneficiaries. These may include managing transitions between care settings, health coaching to improve patient confidence, medication adherence, and an emphasis on preventive and primary care.32 These kinds of efforts can help patients overcome a human tendency called hyperbolic discounting, which causes patients to put off tasks that have long-term benefits.33
One example of the care coordination model is the Better Care Programs (BCPs) envisioned under Senator Ron Wyden’s (D-OR) Better Care, Lower Cost Act.34 Wyden’s BCPs would manage the full scope of a dual eligible beneficiary’s Medicare and Medicaid benefits, with the exception of long-term care. While the Better Care, Lower Cost Act carves out the delivery of long-term care, we would include long-term services and support in the care coordination program to better coordinate the full continuum of health care services a dual eligible beneficiary may utilize.
Other kinds of care coordination plans could include a mix of approaches. It could be a private health plan that takes full financial responsibility for the care of its members, which is a common approach in the CMS demonstration programs. Alternatively, a public plan could assume the costs while still contracting with private organizations that provide coordination. Colorado has adopted this model in its demonstration program.
A consumer advocacy organization, Community Catalyst, rightly notes that the best way to ensure strong enrollment is “to offer robust benefits and high quality health plans that are attractive to consumers because they meet consumer needs in ways the current system does not.”35 While the Capitated Financial Alignment Demonstration permits automatic enrollment of beneficiaries into care coordination programs, the idea has caused concern among patients and patient advocacy groups. Our proposal is different, and includes the following steps:
First, we would begin with a voluntary open enrollment period. In states with only one alternative to current coverage, beneficiaries could switch to the new coverage anytime. Once multiple care coordination options were available in a state, beneficiaries who do not enroll in a program after the voluntary open enrollment would be automatically enrolled in the highest-quality, lowest-cost option appropriate for the beneficiary’s health needs and that demonstrates capacity and competency readiness. The basis for determining the highest-value plan would be half from quality rating score and the other from the cost of coverage (cost to the government, not beneficiary, since duals do not pay a portion of the premium).
Second, in order to ensure that private health plans or care management programs have the capacity to serve all beneficiaries who are automatically enrolled in their plans, the states or federal government could phase-in enrollment over a three- to four-year period, using geographic area, beneficiary date of birth, or other factors. Furthermore, this phased-in automatic enrollment would begin with beneficiaries who have less complex health care needs.36
Third, any enrollment in a coordinated plan would include the option for the beneficiary to change enrollment for any reason within the first three months after initial enrollment. Beneficiaries would also have a chance to change plans during an annual open enrollment period. A yearly enrollment commitment gives the plan an opportunity to make and recoup investments in preventive and primary care measures for each beneficiary. However, beneficiaries’ requests to change plans could be granted at any time if they have problems such as getting access to care. Third party, in-person assisters, such as community-based organizations that already work with duals, would be available to assist beneficiaries during open enrollment, review the plan into which a beneficiary was automatically enrolled, and assist beneficiaries with selection of another plan, if they so desire.
Finally, either the state or the federal government would take full responsibility for coordinating care for the duals with financing aligned under the responsible government. Each state would have right of first refusal to establish care coordination programs for its dual eligible beneficiaries and receive payment from the federal government for the Medicare portion of their care. If a state does not elect this option, the federal government would take responsibility for coordinating care for dual eligible beneficiaries in that state through Sen. Wyden’s Better Care Program. Under this option, the state would make a payment to the federal government for the Medicaid portion of their care, as outlined in the Better Care, Lower Cost Act.37
As in the CMS demonstrations, states and private sector stakeholders should be rewarded for leading and financing the care coordination by sharing the savings that will accrue to Medicare. Should a state take responsibility for coordinating the care of dual eligible beneficiaries, one model for distribution of any savings is gain sharing—a partnership between the federal government, private sector stakeholders, and the states that recognizes actions taken by one sector may result in the accrual of savings to another sector.38 Our proposal would require Congress to set up a method for sharing savings that accrue to Medicare with states that choose to take the lead in coordinating care for dual eligible beneficiaries. States may then choose to share their portion of the savings to make investments in upfront costs that can produce savings and better health outcomes down the road. States could also choose a more predictable, but likely smaller fixed percentage savings rate as they can under the CMS Financial Alignment Demonstrations. States would have to be part of periodic federal reviews to determine if they are providing actuarially sound payments.
Potential Savings
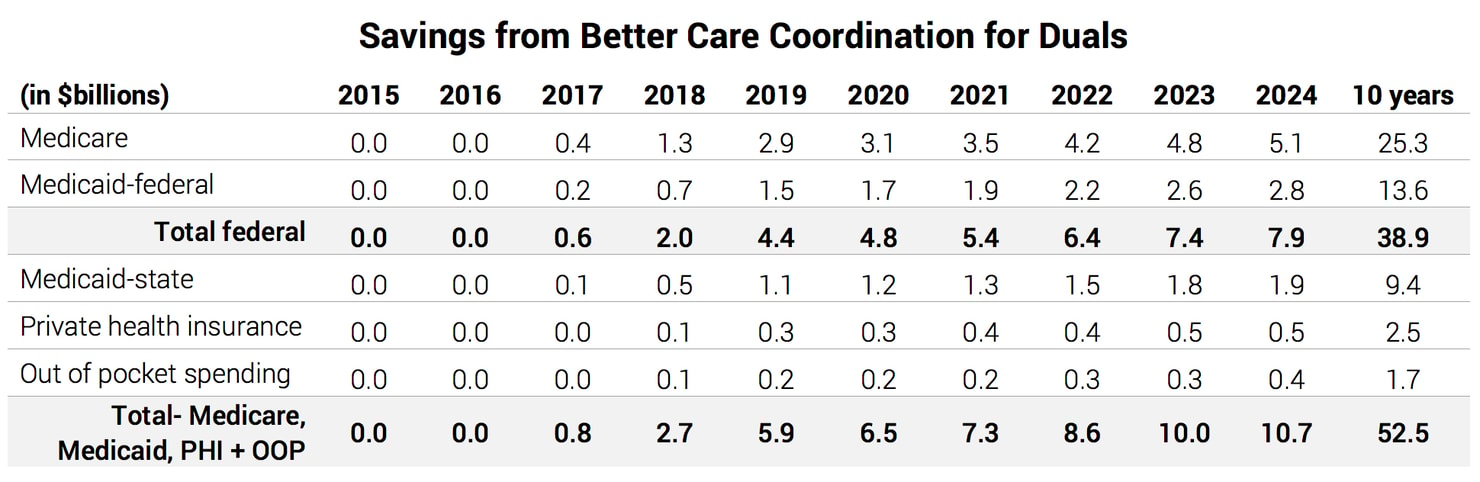
Federal savings from this proposal would be $38.9 billion over 10 years.39 The savings come from coordinating benefits between Medicare and Medicaid, which would eliminate care that is duplicated between the two programs and also fill gaps in care that can reduce costs across both programs. The estimated savings are based, in part, on the managed care contract prices in states that are participating in the Capitated Financial Alignment Demonstration.
The year-by-year savings shown in the chart below do not start until 2017 for two reasons. First, this proposal would take effect in states after their current demonstration programs end over the next three years. Second, the estimate of savings assumes that it will take at least one year of full operation in coordinate Medicare and Medicaid benefits to realize savings on a broad scale. This savings estimate falls within the range of estimates of other proposals that would save from $12 billion over ten years40 to $70 billion over 15 years.41
Questions and Responses
How would funds transfers between states and the federal government work?
Under this proposal, one of two different transfers may occur, depending on each state’s choice.
First, in states that choose to establish care coordination programs for dual eligible beneficiaries, the federal government would provide the state with a payment for the Medicare portion of each dual eligible beneficiary’s care based on the Medicare Advantage payment structure, with some notable changes. The federal government would establish a new benchmark rate for dual eligible beneficiaries to reflect their higher costs. States would collect county- or region-level bids from managed care organizations and choose the lowest cost, high quality plan or plans with which to contract. The difference between the benchmark and the bid is savings that would accrue to the Medicare program, and would be shared by Medicare and the state (see below).42
Payments to states would then be adjusted for risk and for frailty, using a combination of Medicare Advantage and PACE program adjustors in an effort to more accurately reflect the duals’ cost of care. Payments would be adjusted according to the Medicare Advantage risk adjustment system which uses enrollees’ demographics and health conditions, organized into 70 hierarchical condition categories, to predict the cost of each enrollee’s care.43 In addition, payments would reflect the 2012 refinements to the PACE risk adjustment model, which include dementia as a condition. Finally, as in the PACE program, payments would be further adjusted at the contract level to reflect beneficiary frailty.
Second, in states that defer care coordination responsibilities to the federal government, the state would make a payment to the federal government for the Medicaid portion of the dual eligible beneficiaries’ care. Here, Senator Wyden’s Better Care, Lower Cost Act offers a model, based on the Medicare Part D phased-down State contribution (also known as the “clawback”).44
How would Medicare savings be shared with states?
For states that take the lead in coordinating care for dual eligible beneficiaries, savings that accrue to Medicare will be shared with a state in proportion to that state’s share of Medicaid spending. For example, if a state’s Federal Medical Assistance Percentage (FMAP) is 70% and the state’s share is 30%, the state would receive $0.30 of every dollar in Medicare savings.
For states that opt to integrate fee-for-service Medicare and Medicaid, contracts with a care management entity would include performance metrics designed to generate enough Medicare savings to cover the cost of the contract. Any additional savings would be shared with states.

